Wednesday, December 21, 2022
Sunday, December 11, 2022
Anthony Fauci: A Message to the Next Generation of Scientists
… At 81, I still can clearly recall the first time I drove onto the bucolic N.I.H. campus in Bethesda, Md., in June of 1968 as a 27-year-old newly minted physician who had just completed residency training in New York City. My motivation and consuming passion at the time were to become the most highly skilled physician I could, devoted to delivering the best possible care to my patients. This remains integral to my identity, but I did not realize how unexpected circumstances would profoundly influence the direction of my career and my life. I would soon learn to expect the unexpected.
I share my story, one of love of science and discovery, in hopes of inspiring the next generation to enter health-related careers — and to stay the course, regardless of challenges and surprises that might arise…
https://www.nytimes.com/2022/12/10/opinion/anthony-fauci-retirement.html?smid=nytcore-ios-share&referringSource=articleShare
Anthony Fauci: A Message to the Next Generation of Scientists
Anthony Fauci: A Message to the Next Generation of Scientists
We Can Cure Disease by Editing a Person’s DNA. Why Aren’t We?
But for the next few years, devastating genetic ailments and cancer are where CRISPR clinical trials must remain; ethical considerations over the safety of patients being exposed to new technology dictate that. Today's tools are also the cognate of the first iPod — at the time, an exhilarating advance but still low tech compared with present-day smartphones. Everything we learn about how to gene-edit people from this work, coupled with continued CRISPR innovation in the academic and for-profit sector, will provide a foundation for more deeply understanding how to safely edit DNA to treat and potentially prevent dire common diseases.
The invention of CRISPR gene editing gave us remarkable treatment powers, yet no one should do a victory lap. Scientists can rewrite a person's DNA on demand. But now what? Unless things change dramatically, the millions of people CRISPR could save will never benefit from it. We must, and we can, build a world with CRISPR for all.
https://www.nytimes.com/2022/12/09/opinion/crispr-gene-editing-cures.html?smid=nytcore-ios-share&referringSource=articleShare
We Can Cure Disease by Editing a Person's DNA. Why Aren't We?
We Can Cure Disease by Editing a Person's DNA. Why Aren't We?
Wednesday, November 9, 2022
Friday, October 21, 2022
Much Work Remains
| ||||||||||||||||||||||||
Wednesday, October 19, 2022
The neglected clitoris
Half the World Has a Clitoris. Why Don't Doctors Study It?
https://www.nytimes.com/2022/10/17/health/clitoris-sex-doctors-surgery.html?smid=nytcore-ios-share&referringSource=articleShare
https://www.nytimes.com/2022/10/17/health/clitoris-sex-doctors-surgery.html?smid=nytcore-ios-share&referringSource=articleShare
Sunday, October 2, 2022
America Is Choosing to Stay Vulnerable to Pandemics - The Atlantic
Recently, after a week in which 2,789 Americans died of COVID-19, President Joe Biden proclaimed that "the pandemic is over." Anthony Fauci described the controversy around the proclamation as a matter of "semantics," but the facts we are living with can speak for themselves. COVID still killsroughly as many Americans every week as died on 9/11. It is on track to kill at least 100,000 a year—triple the typical toll of the flu. Despite gross undercounting, more than 50,000 infections are being recorded every day. The CDC estimates that 19 million adults have long COVID. Things have undoubtedly improved since the peak of the crisis, but calling the pandemic "over" is like calling a fight "finished" because your opponent is punching you in the ribs instead of the face...
https://www.theatlantic.com/health/archive/2022/09/covid-pandemic-exposes-americas-failing-systems-future-epidemics/671608/
Scientists Knew More About Covid-19 Than We Think. And They Still Do.
"Nobody," Donald Trump claimed in a March 2020 address, "had any idea." He was talking about the Covid virus — which had, seemingly overnight, sparked a global pandemic. In his compelling and terrifying new book, "Breathless: The Scientific Race to Defeat a Deadly Virus," the veteran science journalist David Quammen demonstrates just how much was known — and expected — by infectious disease scientists long before patrons of the Huanan Seafood Wholesale Market fell ill in December 2019 with a pneumonia-like virus.
"Soothsayer" isn't on Quammen's extensive résumé, but he was among those who had long predicted this kind of catastrophe. In 2012 he provided a field guide to the future, "Spillover," whose subtitle — "Animal Infections and the Next Human Pandemic" — explains exactly what the scientific community had long been expecting.
"This is a book about the science of SARS-CoV-2," he specifies in his new book. "The medical crisis of Covid-19, the heroism of health care workers and other people performing essential services, the unjustly distributed human suffering, and the egregious political malfeasance that made it all worse — those are topics for other books." Instead, he focuses his informed attention on the unsung heroes who dare to wrestle with viruses, those strange entities he calls "the dark angels of evolution." Human beings are part of a sprawling family of interconnected species who can share illness because they all grew up together. It is our common ancestry and related bodily ecology that makes spillover possible between, say, bats and Earth's (currently) dominant mammal.
Covid is, after all, as natural as a wolf cub or David Attenborough, and its thriller-level rate of evolution is part of its danger. "A virus is a parasite, yes," writes Quammen, "a genetic parasite, to be more precise, using the resources of other organisms to replicate its own genome." He demonstrates the sheer weirdness of viruses when he explains how difficult it is to even define them...
Thursday, September 29, 2022
Tweet by NPR on Twitter
| ||||||||||||||||||||||||
Tuesday, September 20, 2022
‘Very Harmful’ Lack of Data Blunts U.S. Response to Outbreaks
'Very Harmful' Lack of Data Blunts U.S. Response to Outbreaks
Major data gaps, the result of decades of underinvestment in public health, have undercut the government response to the coronavirus and now to monkeypox.
https://www.nytimes.com/2022/09/20/us/politics/covid-data-outbreaks.html?smid=nytcore-ios-share&referringSource=articleShare
Sunday, August 21, 2022
Her Discovery Changed the World. How Does She Think We Should Use It?
…What about the ethics of all those gene-editing possibilities? That's something you've been talking about for years now, but what would it look like to actually resolve those ethical issues? What is the green light we'd be waiting for that would make us say, "This form of gene editing was not OK yesterday, but it is OK today?" Maybe let's start with, "Where are the ethical boundaries right now for CRISPR technology?" Two come to mind…
3
https://www.nytimes.com/interactive/2022/08/15/magazine/jennifer-doudna-crispr-interview.html?smid=nytcore-ios-share&referringSource=articleShare But at the same time it could clearly have environmental impacts that might be of concern. That's one aspect. The other is using CRISPR in the human germ line. Meaning making changes in embryos that, if implanted to create a pregnancy, then would create human beings who have edits to their DNA that are not just affecting them but can also be passed on to future generations. Those are two distinct applications, but it's fairly clear why both of those could have profound impacts that could be dangerous. Understanding that, and then thinking about how to proceed as the technology continues to advance, has been incredibly important. Let's take the human-embryo example. Is there a particular event or decision or developments that would suddenly make us say, "Oh, we didn't think it was OK yesterday, but now it seems fine?" No. But it's a complex issue. There would be technical considerations. In other words, even before we ask, "Should we do this?" we have to ask, "Can it be done accurately and safely in a way that creates a change that is desired by the scientist who's doing the work?" Right now that's still not true in human embryos, I would say.
Sunday, August 14, 2022
A huge side benefit of the new climate bill
Air pollution sickens and kills millions every year. Here’s how the new measure will help tackle the problem.
...the law will avert heart attacks, lower emergency room visits of people suffering from respiratory problems and reduce hospital admissions by people with cardiovascular disease...
https://www.nytimes.com/2022/08/12/climate/climate-air-pollution-health.html?smid=em-share
Saturday, July 23, 2022
Why Storytelling Is Part of Being a Good Doctor
Doctors are people too.
"…the word 'doctor' comes from the Latin 'to teach.' By writing stories, we as doctors aim to teach others about our patients while learning about ourselves."
https://www.newyorker.com/magazine/2022/07/25/why-storytelling-is-part-of-being-a-good-doctor-all-that-moves-us-jay-wellons
Sunday, July 17, 2022
Time for a national public health system
Since the early months of the covid-19 pandemic, it's been clear that the U.S. public health system needs major improvements. Now, a blue-ribbon commission assembled by the Commonwealth Fund has issued a reportwith a rather provocative conclusion: The United States needs a Since the early months of the covid-19 pandemic, it's been clear that the U.S. public health system needs a national public health system.... Leana Wen
https://www.washingtonpost.com/opinions/2022/07/05/is-it-time-national-public-health-system/
Wednesday, July 13, 2022
BCSP/HT Change Your Mind
Berkeley Center for the Science of Psychedelics
Friends, readers, viewers,
I’m happy to share that the four-part Netflix series based on How to Change Your Mind is streaming beginning today.
 |
I’m grateful to the whole crew at Jigsaw Productions for their brilliant work in bringing the book to the screen. You can read a review of the series here.
I’m also pleased to announce the launch, today, of a new psychedelic resources website from the Berkeley Center for the Science of Psychedelic (BCSP). The inspiration for the website was our concern that the Netflix series would create a wave of interest and curiosity about psychedelic therapy. We decided that it would be helpful if these viewers had a one-stop site that could answer their questions—including descriptions of the various substances; their risks and benefits; advice for people seeking psychedelic therapy, and much more, all written and edited by a team of journalists.
Thanks to the crew at the BCSP, as well as the teams at Pentagram and Wordpress, for the inspired work that went into building the site.
I hope you’ll get a chance to explore the site as well as watch the series. Do let me know what you think!
Best,
Michael Pollan
 |
Friday, July 8, 2022
CRISPR cure for sickle cell
nearly 100% effective after three years
Newly released data shows nearly universal efficacy with no
drop in effectiveness.
June
25, 2022
When CRISPR Therapeutics
and Vertex used gene editing to try to cure heritable blood disorders in 2019,
it marked the first CRISPR trial outside
of China.
A year later, the trial
— using the CRISPR gene editor to treat sickle cell disease and beta
thalassemia — showed promising results, Freethink reported in
2020.
Now, three years after
the trial began, the researchers have presented new data showing that the
treatment continues to be effective.
“These data provide
further evidence that this treatment has the potential to be transformational
for patients with sickle cell disease and beta thalassemia,” trial abstract author
Stephan A. Grupp of the Children’s Hospital of Philadelphia said in a statement.
New
data shows that the CRIPR sickle cell and beta thalassemia treatment continues
to be effective even three years out.
The diseases: Severe
sickle cell disease (SCD) and transfusion-dependent beta thalassemia (TDT) are
both caused by genetic mutations impacting hemoglobin, the molecule red blood
cells use to carry oxygen throughout the body.
In SCD, atypical
hemoglobin causes the red blood cells to twist out of shape, contorting into
crescents — or sickles — that cannot deliver oxygen as well. The disease can
cause tiredness and shortness of breath, and periodic sickle cell crises cause
intense pain.
In TDT, patients do not
produce enough hemoglobin at all, sometimes requiring repeated blood
transfusions, which have their own risks and side effects.
Both can be treated by a
stem cell transplant from a suitable donor, which not only requires finding a good
match but may also require suppressing the patient’s immune system.
The therapy: The
CRISPR treatment, originally dubbed CTX001 and now called exa-cel, is a
one-time treatment that genetically alters the patient’s own cells to produce
the kind of hemoglobin found at birth, which isn’t distorted, allowing red
blood cells to work properly.
The new data, presented
at the European Hematology Association Congress but yet to be published in a
peer-reviewed journal, reported results from 75 patients.
Of the TDT patients, 42
out of 44 were blood transfusion-free up to 37.2 months after their exa-cel
infusion, according to CRISPR Therapeutics and
Vertex. They are essentially cured of
the disease.
The
CRISPR therapy is a one-time treatment that genetically alters the patient’s
own cells.
The remaining two
patients needed much less transfusion volume, and all of the TDT patients had
elevated levels of fetal hemoglobin and total hemoglobin in their blood.
All of the SCD patients
were free from sickle cell attacks, up to 32.3 months later.
Two of the TDT patients
suffered adverse effects possibly related to exa-cel, including delayed growth
of white blood cells and a low blood platelet count, both of which resolved on
their own.
Importantly, the team
found no evidence of exa-cel’s effectiveness waning over time, even three years
after infusion.
“Although we must
continue to investigate the durability of these results, I am excited about the
current data,” Grupp said.
Friday, June 3, 2022
Authors Michael Lewis and Malcolm Gladwell | C-SPAN.org
Michael Lewis on The Premonition—
https://www.c-span.org/video/?518489-2/authors-michael-lewis-malcolm-gladwell
https://www.c-span.org/video/?518489-2/authors-michael-lewis-malcolm-gladwell
Sunday, May 29, 2022
Australia’s solution
| ||||||||||||||||||||||||
Sandy Hook to Uvalde
| ||||||||||||||||||||||||
The Anti-Vaccine Movement’s New Frontier
A wave of parents has been radicalized by Covid-era misinformation to reject ordinary childhood immunizations — with potentially lethal consequences.
https://www.nytimes.com/2022/05/25/magazine/anti-vaccine-movement.html?referringSource=articleShare
Anti-vax, an old story
| ||||||||||||||||||||||||
Sunday, May 15, 2022
How
Public Health Failed America
The U.S. clearly failed to heed expert advice,
but there’s plenty of blame to go around.
By Jay
Varma
MAY 15, 2022, 7
AM ET
https://www.theatlantic.com/ideas/archive/2022/05/how-public-health-failed-america/629869/
About the
author: Jay Varma, a professor
at Weill Cornell Medical School, is a physician and epidemiologist who worked
for the CDC in New York, Bangkok, Beijing, and Addis Ababa.
Even
though anthony Fauci, the White
House’s chief medical adviser, backed off his statement that the United States
is “out of the pandemic phase,” elected officials and much of the public seem
to think that he had it right the first time. But if the end of the COVID-19
emergency is at hand, the United States is reaching it with lower vaccination
and higher per capita death rates than other wealthy nations. The conventional
wisdom is that the American political system failed at public health—by
prioritizing individual rights over collective safety; sowing doubt about the
benefits of vaccines, masks, and other protective measures; and most important,
failing to implement universal health care, paid sick leave, and other
safety-net programs.
I agree with the conventional wisdom. But
there’s plenty of blame to go around. Public health also failed America. The
two most important federal public-health agencies, the CDC and the FDA, have been uniformly criticized for muddled
messaging and guidance to the public on masks, vaccines, rapid tests, and other
matters; those arguments need no rehashing here. Less well understood is that
other sectors of our public-health system—including local agencies and
prominent public-health academics—were unprepared for a nationwide
infectious-disease emergency, particularly in a divided country with tight
limits on government power.
As federal, state, and local health officials
struggled in spring 2020 to obtain the basic funding, staff, lab supplies, and
data systems to test, trace, and isolate cases, academics on Twitter and cable
news became the face of public health—and they zeroed in on the many ways in
which the U.S. response to COVID-19 fell short of a textbook approach to
pandemic control. Public-health agencies were ill-prepared for this crisis, and
academics were ill-prepared to speak on their behalf.
The U.S. has a highly decentralized
public-health system that relies on thousands of state and local health
agencies operating with a wide degree of independence. The origin of these
agencies lies in combatting malaria, yellow fever, smallpox, syphilis, and
other infectious diseases; their standard activities historically included
controlling mosquitoes, improving water quality and sanitation, isolating and
quarantining people during disease outbreaks, and the direct provision of
prevention and treatment services.
By the mid-20th century, though, heart disease,
lung disease, cancer, and other chronic conditions replaced infectious diseases
as the leading causes of death. Over several decades, public-health agencies
reduced their focus on environmental dangers, infectious disease, and clinical
services. In the 2000s, these agencies dedicated more and more personnel and
public communications to tobacco control, promoting physical activity and
healthy diets, and screening for diabetes, heart disease, and cancer. The
consensus of government and academic public-health experts was that the most
effective way for these agencies to serve the public was to reduce illness and
death from chronic disease. The key metric for judging the effectiveness of
public-health agencies was life expectancy in the community they served, and—at
least in the immediate pre-COVID era—promoting healthy lifestyles for all was
more likely to avert premature deaths than infectious-disease control was.
In theory, public-health agencies could add
chronic-disease control activities without sacrificing their infectious-disease
expertise. In reality, however, public-health departments have experienced
a progressive decline in real spending power,
particularly since the Great Recession, and as a result, have chosen to cut
infectious-disease programs. More than 75 percent of the nation’s larger health
departments reported eliminating clinical services from 1997 to 2008.
I experienced this shift firsthand. When I began
overseeing infectious diseases at New York City’s health department in 2011, I
worked for one of the nation’s leading proponents of chronic-disease control:
Mayor Michael Bloomberg. Because of budget cuts, we had to shrink our infectious-diseases
programs; I had to close or reduce hours for our immunization,
sexually-transmitted disease, and tuberculosis clinics. I had to justify these
decisions to appropriately disgruntled community groups and
city council members by saying that the Affordable Care Act’s Medicaid
expansion would pay to ensure that these services could be provided by the
private sector—a claim that I based more on hope than evidence.
As local health agencies nationwide scaled back
their clinics, they also lost their presence in the community. Clinics are an
important way of building visibility and credibility, because most people do
not understand what a public-health agency is or does. Residents see the good
work you do, tell elected officials that your work matters, and then trust you
during emergencies. Running clinics also builds logistical expertise.
Unfortunately, when health agencies were called
on to run the largest, most rapid vaccination campaign in U.S. history, most
lacked personnel qualified to either run these clinics themselves or oversee
contractors effectively. This resulted in debacles like the one in Philadelphia, where the
health department let an untested start-up take on the job of running
mass-vaccination clinics in the city. Public-health agencies lost an
opportunity: One way to overcome vaccine hesitancy is to have trusted providers
deliver information and services. Without a strong public presence directly
administering vaccines before the pandemic, local health departments were
additionally unprepared to reach communities inherently distrustful of a
mass-vaccination campaign.
The U.S. is not as different from the rest of
the world as Americans frequently think. After the 2002–04 SARS epidemic and
the 2014–16 Ebola epidemic in West Africa, independent reviewers of the World Health
Organization concluded that the agency had become too
focused on providing high-level technical guidance and had failed to invest in
staff and systems to respond quickly during emergencies. During the COVID-19
crisis, the agency has been far more effective than during past crises in
mobilizing personnel and supplies in all regions of the world for border
screening, laboratory testing, and vaccination. The crucial lesson that WHO learned
from the earlier epidemics is that failure to rapidly and effectively solve
urgent problems, such as infectious-disease outbreaks, destroys your
credibility and prevents you from addressing the long-term problems and leading
causes of death. Imagine a fire department that was focused on reducing the
frequency of kitchen burns and not on putting out infernos in high-rise
buildings. That’s the situation that local public-health officials found
themselves in.
For
most americans, the face of public
health during COVID-19 was not, however, local health officials. The most
prominent voices—other than Anthony Fauci’s—were university professors
proffering guidance on television, in print, and through social media. People
who practice public health in government are expected to stick to the talking
points for their agency; the mayor or governor whom they serve constrains them
from freely explaining their recommendations and decisions. Even if afforded
freedom to talk more openly, they lacked the time to do so.
Into that void stepped university-based
physicians, epidemiologists, and virologists opining about what the government
should do without fully understanding or communicating what was feasible,
affordable, legal, and politically acceptable for public-health agencies. When
I was advising New York City Mayor Bill de Blasio on how to respond to COVID in
2020 and 2021, the city faced terrible choices. As we attempted to return the
country’s largest school district to in-person instruction in the fall of 2020
and then to keep classrooms open in the following months, I had to parse
uncertain science while balancing the demands of staff unions, parents, and
elected officials. Meanwhile, experts publicly faulted us for our limited ability to identify the source of infection for
any given COVID case and for our failure to test every COVID-exposed student every day.
Anyone who had actually implemented a large testing-and-contact-tracing program
understood the impossibility of such demands. But most of the people with
genuine technical expertise were busy practicing public health, not doing multiple
cable-news hits a day.
Consumers of that commentary could easily
conclude that the government was simply not trying hard enough to stop the
virus. And yet state and local health agencies generally cannot remove the
major legal, financial, and political constraints they face. For example, critics faulted the CDC and local health
agencies for not releasing enough data, but didn’t acknowledge the strict,
complex patchwork of regulations at the federal and state level that limit what
data public-health agencies can legally receive and report.
Every public-health practitioner I know
understands that the U.S. can reduce its vulnerability to epidemics by
improving data collection. Likewise, most of my colleagues believe that
strengthening the social safety net—particularly through universal health care,
paid sick leave, housing, and child care—will improve Americans’ ability to
fend off COVID-19 and other threats. But enacting those measures is beyond the
power of public-health officials, whose job it is to mitigate harm under
real-world conditions. Those conditions include the underlying laws and systems
that elected officials created.
Universities and government agencies are subject
to different prerogatives. The economic model of public-health schools rewards
professors who bring in research grants; tenure committees and research funders
do not necessarily demand that professors have experience inside government
public-health agencies. In reporting the comments of academic experts, news
outlets routinely include their university affiliation. But other credentials
are more crucial: Have you ever run a large government health program?
Have you ever led an official outbreak investigation? Academic experts
can offer the public an idealized version of what public health could be, but
during this pandemic they have also played a role in setting unrealistic
expectations—for instance, that emergency measures could go on indefinitely,
until society’s underlying failures are addressed.
I don’t mean to be too critical of my academic
colleagues. (Full disclosure: I now teach at a university too.) The greatest
threats to public health right now come from elected officials who would gut
public-health agencies’ budgets and legal authority on the grounds that they
threaten individual liberties.
One way to avoid that fate is for health leaders
to recognize that their daily work is largely invisible to the general
public—and that the public expects health agencies to focus on threats that
they do not believe they can protect themselves from. Public-health experts,
both in academia and in government, rightly point out that the holes in
social-welfare policies are the primary determinants of ill health. These
experts also believe that, for instance, promoting healthy diets and
encouraging people to wear masks are worthy goals of government policy. But most
Americans, for better or worse, still prioritize individual choice more and
community protection less than those of us drawn to the public-health field do.
To rally voters’ support, agencies need to make
themselves more visible in public life through direct clinical services and
ensure that they are dedicating sufficient resources, even within constrained
budgets, to public-health-emergency response. Meanwhile, the interested voter
should press elected officials on their plans for restoring infectious-disease
and emergency-response services. Ultimately, the highest aspirations of the
public-health profession must coexist with the reality of law and where power
actually resides in a democracy: with voters and their elected representatives.
Jay Varma, a professor
at Weill Cornell Medical School, is a physician and epidemiologist who worked
for the CDC in New York, Bangkok, Beijing, and Addis Ababa.
Saturday, May 14, 2022
How America Reached One Million Covid Deaths
THE MAGNITUDE OF THE country's loss is nearly impossible to grasp.
More Americans have died of Covid-19 than in two decades of car crashes or on battlefields in all of the country's wars combined.
Experts say deaths were all but inevitable from a new virus of such severity and transmissibility. Yet, one million dead is a stunning toll, even for a country the size of the United States, and the true number is almost certainly higher because of undercounting.
It is the result of many factors, including elected officials who played down the threat posed by the coronavirus and resisted safety measures; a decentralized, overburdened health care system that struggled with testing, tracing and treatment; and lower vaccination and booster rates than other rich countries, partly the result of widespread mistrust and resistance fanned by right-wing media and politicians.
The virus did not claim lives evenly, or randomly. The New York Times analyzed 25 months of data on deaths during the pandemic and found that some demographic groups, occupations and communities were far more vulnerable than others. A significant proportion of the nation's oldest residents died, making up about three-quarters of the total deaths. And among younger adults across the nation, Black and Hispanic people died at much higher rates than white people.
Understanding the toll — who makes up the one million and how the country failed them — is essential as the pandemic continues. More than 300 people are still dying of Covid every day.
"We are a country with the best doctors in the world, we got a vaccine in an astoundingly short period of time, and yet we've had so many deaths," said Mary T. Bassett, the health commissioner for New York State.
"It really should be a moment for us all to reflect on what sort of society we want to have..."
https://www.nytimes.com/interactive/2022/05/13/us/covid-deaths-us-one-million.html
More Americans have died of Covid-19 than in two decades of car crashes or on battlefields in all of the country's wars combined.
Experts say deaths were all but inevitable from a new virus of such severity and transmissibility. Yet, one million dead is a stunning toll, even for a country the size of the United States, and the true number is almost certainly higher because of undercounting.
It is the result of many factors, including elected officials who played down the threat posed by the coronavirus and resisted safety measures; a decentralized, overburdened health care system that struggled with testing, tracing and treatment; and lower vaccination and booster rates than other rich countries, partly the result of widespread mistrust and resistance fanned by right-wing media and politicians.
The virus did not claim lives evenly, or randomly. The New York Times analyzed 25 months of data on deaths during the pandemic and found that some demographic groups, occupations and communities were far more vulnerable than others. A significant proportion of the nation's oldest residents died, making up about three-quarters of the total deaths. And among younger adults across the nation, Black and Hispanic people died at much higher rates than white people.
Understanding the toll — who makes up the one million and how the country failed them — is essential as the pandemic continues. More than 300 people are still dying of Covid every day.
"We are a country with the best doctors in the world, we got a vaccine in an astoundingly short period of time, and yet we've had so many deaths," said Mary T. Bassett, the health commissioner for New York State.
"It really should be a moment for us all to reflect on what sort of society we want to have..."
https://www.nytimes.com/interactive/2022/05/13/us/covid-deaths-us-one-million.html
Wednesday, May 11, 2022
Can Anyone Out-Plan a Pandemic?
Bill Gates has a strategy to save the world from the next infectious threat. He’s not the first.
...To believe that you need only a plan rests on an assumption that humans are rational creatures who have roughly the same values and priorities as you do, and—even more improbable—that humans are inclined to follow plans of any kind. After all, when Gates laid out a strategy for solving climate change last year, he was boldly going where world leaders had gone many, many times before without success. The United Nations has held no fewer than 26 annual climate-change conferences. The world committed to the Kyoto Protocol in 1997, but failed to meet its goals. The Paris Agreement is seven years old, and the UN itself says we’re falling short. But Gates told me that the plan he offered in How to Avoid a Climate Disaster has already done some good for the planet...
https://www.theatlantic.com/science/archive/2022/05/bill-gatess-plan-save-world-next-pandemic/629826/?utm_source=email&utm_medium=social&utm_campaign=share
Friday, May 6, 2022
Our Obsession with Ancestry Has Some Twisted Roots
...Today’s addictive Web sites and sleekly packaged DNA kits rest on deep, if not always acknowledged, assumptions about the fixity of status, race, ethnicity, and nationality... NYer
Wednesday, May 4, 2022
Something in the Way We Move
We may each have a movement "signature" that, like our face or fingerprints, is unique to us.
Each of us appears to have a unique way of moving, a physical "signature" that is ours alone, like our face or fingerprints, according to a remarkable new study of people and their muscles. The study, which used machine learning to find one-of-a-kind patterns in people's muscular contractions, could have implications for our understanding of health, physical performance, personalized medicine and whether and why people can respond so differently to the same exercise.
Intuitively, most of us probably know there is something in the way we move, and that that something defines us. In studies and daily life, most people can pick out their friends and loved ones, based solely on how they walk. At least one surveillance company also claims to be able to identify and track people using their gaits... nyt
Each of us appears to have a unique way of moving, a physical "signature" that is ours alone, like our face or fingerprints, according to a remarkable new study of people and their muscles. The study, which used machine learning to find one-of-a-kind patterns in people's muscular contractions, could have implications for our understanding of health, physical performance, personalized medicine and whether and why people can respond so differently to the same exercise.
Intuitively, most of us probably know there is something in the way we move, and that that something defines us. In studies and daily life, most people can pick out their friends and loved ones, based solely on how they walk. At least one surveillance company also claims to be able to identify and track people using their gaits... nyt
Monday, May 2, 2022
Sunday, May 1, 2022
Racial disparities in US healthcare
| ||||||||||||||||||||||||
Friday, April 29, 2022
FINAL POST: The Ethics of Harm Reduction
Hi everyone! Today we will be speaking about harm reduction.
Harm reduction offers a “pragmatic yet compassionate set of strategies designed to reduce the harmful consequences of addictive behavior for both drug consumers and the communities in which they live.” (Marlatt)
So what are some examples of harm reduction you can think of?
One example that I think of is having a designated driver when a group of people attend a party where there will be alcohol. Another one I can think of is teaching children about condom use during sex education. Even seatbelts are an example of harm reduction!
While harm reduction is a rather broad topic and can relate to many different areas, I will be focusing on harm reduction as it relates to substance use, with a specific focus on opioid drug use.
So, we’re talking about reducing potential harms, but what exactly are these harms associated with drug use? Keep in mind that these harms affect not only the individual but society as well. We can divide them up into direct and indirect harms. Direct harms are more what affects strictly that person’s health while indirect harms have more to do with society and situation.
Direct
Harm reduction offers a “pragmatic yet compassionate set of strategies designed to reduce the harmful consequences of addictive behavior for both drug consumers and the communities in which they live.” (Marlatt)
So what are some examples of harm reduction you can think of?
One example that I think of is having a designated driver when a group of people attend a party where there will be alcohol. Another one I can think of is teaching children about condom use during sex education. Even seatbelts are an example of harm reduction!
While harm reduction is a rather broad topic and can relate to many different areas, I will be focusing on harm reduction as it relates to substance use, with a specific focus on opioid drug use.
So, we’re talking about reducing potential harms, but what exactly are these harms associated with drug use? Keep in mind that these harms affect not only the individual but society as well. We can divide them up into direct and indirect harms. Direct harms are more what affects strictly that person’s health while indirect harms have more to do with society and situation.
Direct
-substance use disorder
-bloodborne illnesses (HIV, hepatitis C)
-injection-related bacterial infections (local and systemic)
-overdose complications, including death
Indirect
-violence, homicide, property crime
-involvement in the sex trade
-public stigmatization (It is important to avoid using older, stigmatizing terms when discussing this topic: https://www.bmc.org/addiction/reducing-stigma)
-homelessness
-incarceration
While attempting to stop illegal drug use, current policies have also contributed to poverty, mass incarceration, and racial disparities. (Vearrier) Harm reduction is designed to decrease HIV transmission and overdose risk while keeping in mind these consequences.
Now, I will be talking about three types of harm reduction used in the U.S. for injection drug use. The first is OEND, or Opioid Overdose Education and Naloxone Distribution. Naloxone is a narcotic that is an antidote for opioid overdose. It is an opioid antagonist, which means that it binds to the sites that opioids usually bind to. Thus, it can reverse or block any effects of other opioids. The point of this harm reduction strategy is to educate people about overdose prevention, what overdose looks like, and what to do in the case of an overdose.
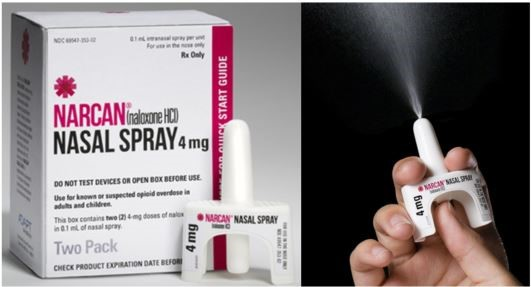
(https://www.co.marion.or.us/HLT/MH/Pages/Narcan-Distribution-Program.aspx)
Next, I’ll talk about the needle and syringe exchange program which many of you have probably heard of before. This program designates sites to collect syringes and dispose of them safely, which is important because diseases such as HIV/AIDS, hepatitis B, and hepatitis C can be spread through this mode. They also provide sterile syringes and other supplies to people. There are 11 official sites in Tennessee and 2 unofficial sites. (Tennessee Harm Reduction)
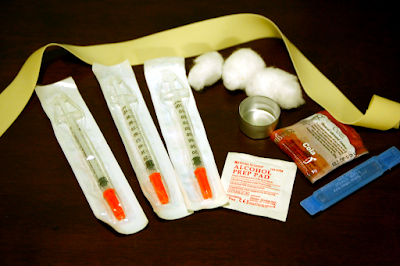 (https://en.wikipedia.org/wiki/Needle_and_syringe_programmes)
(https://en.wikipedia.org/wiki/Needle_and_syringe_programmes)
Now, we'll take a look at opioid maintenance therapy, which is where relatively safer opioids are given to patients who struggle with an opioid use disorder. Methadone and suboxone are longer-acting opiates that are taken orally (safer!). However, a patient can get dependent on both of these, and they do have some street value. There are many regulations in place for these medications to be dispensed. For example, methadone can only be dispensed from specialized clinics, and at the beginning of treatment, patients are actually required to swallow the pills while in the clinic and submit to random urine drug screens and pill counts.
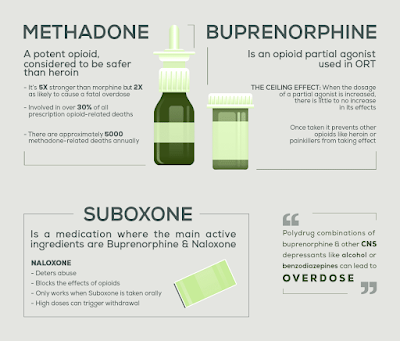
(https://www.northpointrecovery.com/blog/opioid-replacement-therapy-risks-methadone-vs-buprenorphine/)
So now that we’ve talked about these strategies, let’s examine them using the four guiding principles of ethics.
-Autonomy: Yes, we are meeting patients where they are. ("come as you are, and I’ll treat you” & “whether you are using or not, I’ll help you”)
-Beneficence: Yes. This will decrease HIV and overdose risk, doctors get informed consent from patients before prescribing anything, and it decreases the indirect harms associated with drug use.
-Non-maleficence: We could essentially cause harm--a patient could previously be addicted to heroin and now be addicted to or even overdose on methadone. However, we use the equation "total harm = average harm per use x total use" to understand the amount of harm involved. A doctor may have hurt or even led to someone's death with the prescription, but if we look at all the people who have used these opiates and survived many uses because of the prescription, it is good overall.
-Justice: Yes. These harm reduction strategies play a part in eliminating racial disparities and decreasing the amount of people who are incarcerated and houseless.
Now, let’s take this a step further. Let’s talk about two other harm-reduction strategies that are not yet accepted and widely used in the United States. The first is safe injection sites. Basically, safe injection sites provide someone who uses drugs a safe place to come in and use, and there are trained staff present to keep an eye on them. And if they observe signs of overdose, the staff has naloxone on hand and can call for medical help. There are a few of these sites in New York. Per the federal government, the possession of these drugs are illegal, so the sites make a pact with the local law enforcement and agree that these patients will not be prosecuted for possession.

(https://capitalandmain.com/moving-the-needle-science-supports-supervised-injection-sites-why-dont-politicians-agree-1024)
Next, for patients who continue to use heroin despite being prescribed suboxone and methadone, medical-grade heroin can dispensed. There is one site in Canada that does this. What do you guys think about this?
So while the ultimate goal is abstinence, when patients are not able to abstain or are not willing to abstain, rather than ignoring their needs or using punitive measures, harm reduction allows us to meet them where they are and offer some strategies to decrease harm not only to them but also to society.
Some important things to keep in mind are:
1. Getting informed consent
2. Clearly defining the parameters within which these harm reduction strategies will be implemented to minimize risk (train doctors, understand how these treatments work, minimize risk of diversion, minimize risk of overdose)
3. For optimal effects, there may need to be changes to our laws and public opinion so they can go hand-in-hand with the harm reduction strategies we want to implement.
Sources:
Hedrich D, Alves P, Farrell M, Stöver H, Møller L, Mayet S. The effectiveness of opioid maintenance treatment in prison settings: a systematic review. Addiction. 2012 Mar;107(3):501-17. doi: 10.1111/j.1360-0443.2011.03676.x. PMID: 21955033.
Khalid, Farhan et al. “Social Stigmatization of Drug Abusers in a Developing Country: A Cross-Sectional Study.” Cureus vol. 12,9 e10661. 26 Sep. 2020, doi:10.7759/cureus.10661
Marlatt, G.Alan. “Harm Reduction: Come as You Are.” Addictive Behaviors, vol. 21, no. 6, 1996, pp. 779–788., https://doi.org/10.1016/0306-4603(96)00042-1.
Stoljar N. Disgust or Dignity? The Moral Basis of Harm Reduction. Health Care Anal. 2020 Dec;28(4):343-351. doi: 10.1007/s10728-020-00412-y. Epub 2020 Oct 24. PMID: 33098488.
Vearrier L. The value of harm reduction for injection drug use: A clinical and public health ethics analysis. Dis Mon. 2019 May;65(5):119-141. doi: 10.1016/j.disamonth.2018.12.002. Epub 2018 Dec 29. PMID: 30600096.
-bloodborne illnesses (HIV, hepatitis C)
-injection-related bacterial infections (local and systemic)
-overdose complications, including death
Indirect
-violence, homicide, property crime
-involvement in the sex trade
-public stigmatization (It is important to avoid using older, stigmatizing terms when discussing this topic: https://www.bmc.org/addiction/reducing-stigma)
-homelessness
-incarceration
While attempting to stop illegal drug use, current policies have also contributed to poverty, mass incarceration, and racial disparities. (Vearrier) Harm reduction is designed to decrease HIV transmission and overdose risk while keeping in mind these consequences.
Now, I will be talking about three types of harm reduction used in the U.S. for injection drug use. The first is OEND, or Opioid Overdose Education and Naloxone Distribution. Naloxone is a narcotic that is an antidote for opioid overdose. It is an opioid antagonist, which means that it binds to the sites that opioids usually bind to. Thus, it can reverse or block any effects of other opioids. The point of this harm reduction strategy is to educate people about overdose prevention, what overdose looks like, and what to do in the case of an overdose.
(https://www.co.marion.or.us/HLT/MH/Pages/Narcan-Distribution-Program.aspx)
Next, I’ll talk about the needle and syringe exchange program which many of you have probably heard of before. This program designates sites to collect syringes and dispose of them safely, which is important because diseases such as HIV/AIDS, hepatitis B, and hepatitis C can be spread through this mode. They also provide sterile syringes and other supplies to people. There are 11 official sites in Tennessee and 2 unofficial sites. (Tennessee Harm Reduction)
(https://en.wikipedia.org/wiki/Needle_and_syringe_programmes)Now, we'll take a look at opioid maintenance therapy, which is where relatively safer opioids are given to patients who struggle with an opioid use disorder. Methadone and suboxone are longer-acting opiates that are taken orally (safer!). However, a patient can get dependent on both of these, and they do have some street value. There are many regulations in place for these medications to be dispensed. For example, methadone can only be dispensed from specialized clinics, and at the beginning of treatment, patients are actually required to swallow the pills while in the clinic and submit to random urine drug screens and pill counts.
(https://www.northpointrecovery.com/blog/opioid-replacement-therapy-risks-methadone-vs-buprenorphine/)
So now that we’ve talked about these strategies, let’s examine them using the four guiding principles of ethics.
-Autonomy: Yes, we are meeting patients where they are. ("come as you are, and I’ll treat you” & “whether you are using or not, I’ll help you”)
-Beneficence: Yes. This will decrease HIV and overdose risk, doctors get informed consent from patients before prescribing anything, and it decreases the indirect harms associated with drug use.
-Non-maleficence: We could essentially cause harm--a patient could previously be addicted to heroin and now be addicted to or even overdose on methadone. However, we use the equation "total harm = average harm per use x total use" to understand the amount of harm involved. A doctor may have hurt or even led to someone's death with the prescription, but if we look at all the people who have used these opiates and survived many uses because of the prescription, it is good overall.
-Justice: Yes. These harm reduction strategies play a part in eliminating racial disparities and decreasing the amount of people who are incarcerated and houseless.
Now, let’s take this a step further. Let’s talk about two other harm-reduction strategies that are not yet accepted and widely used in the United States. The first is safe injection sites. Basically, safe injection sites provide someone who uses drugs a safe place to come in and use, and there are trained staff present to keep an eye on them. And if they observe signs of overdose, the staff has naloxone on hand and can call for medical help. There are a few of these sites in New York. Per the federal government, the possession of these drugs are illegal, so the sites make a pact with the local law enforcement and agree that these patients will not be prosecuted for possession.
(https://capitalandmain.com/moving-the-needle-science-supports-supervised-injection-sites-why-dont-politicians-agree-1024)
Next, for patients who continue to use heroin despite being prescribed suboxone and methadone, medical-grade heroin can dispensed. There is one site in Canada that does this. What do you guys think about this?
So while the ultimate goal is abstinence, when patients are not able to abstain or are not willing to abstain, rather than ignoring their needs or using punitive measures, harm reduction allows us to meet them where they are and offer some strategies to decrease harm not only to them but also to society.
Some important things to keep in mind are:
1. Getting informed consent
2. Clearly defining the parameters within which these harm reduction strategies will be implemented to minimize risk (train doctors, understand how these treatments work, minimize risk of diversion, minimize risk of overdose)
3. For optimal effects, there may need to be changes to our laws and public opinion so they can go hand-in-hand with the harm reduction strategies we want to implement.
Sources:
Hedrich D, Alves P, Farrell M, Stöver H, Møller L, Mayet S. The effectiveness of opioid maintenance treatment in prison settings: a systematic review. Addiction. 2012 Mar;107(3):501-17. doi: 10.1111/j.1360-0443.2011.03676.x. PMID: 21955033.
Khalid, Farhan et al. “Social Stigmatization of Drug Abusers in a Developing Country: A Cross-Sectional Study.” Cureus vol. 12,9 e10661. 26 Sep. 2020, doi:10.7759/cureus.10661
Marlatt, G.Alan. “Harm Reduction: Come as You Are.” Addictive Behaviors, vol. 21, no. 6, 1996, pp. 779–788., https://doi.org/10.1016/0306-4603(96)00042-1.
Stoljar N. Disgust or Dignity? The Moral Basis of Harm Reduction. Health Care Anal. 2020 Dec;28(4):343-351. doi: 10.1007/s10728-020-00412-y. Epub 2020 Oct 24. PMID: 33098488.
Vearrier L. The value of harm reduction for injection drug use: A clinical and public health ethics analysis. Dis Mon. 2019 May;65(5):119-141. doi: 10.1016/j.disamonth.2018.12.002. Epub 2018 Dec 29. PMID: 30600096.
Subscribe to:
Posts (Atom)