Harm reduction offers a “pragmatic yet compassionate set of strategies designed to reduce the harmful consequences of addictive behavior for both drug consumers and the communities in which they live.” (Marlatt)
So what are some examples of harm reduction you can think of?
One example that I think of is having a designated driver when a group of people attend a party where there will be alcohol. Another one I can think of is teaching children about condom use during sex education. Even seatbelts are an example of harm reduction!
While harm reduction is a rather broad topic and can relate to many different areas, I will be focusing on harm reduction as it relates to substance use, with a specific focus on opioid drug use.
So, we’re talking about reducing potential harms, but what exactly are these harms associated with drug use? Keep in mind that these harms affect not only the individual but society as well. We can divide them up into direct and indirect harms. Direct harms are more what affects strictly that person’s health while indirect harms have more to do with society and situation.
Direct
-substance use disorder
-bloodborne illnesses (HIV, hepatitis C)
-injection-related bacterial infections (local and systemic)
-overdose complications, including death
Indirect
-violence, homicide, property crime
-involvement in the sex trade
-public stigmatization (It is important to avoid using older, stigmatizing terms when discussing this topic: https://www.bmc.org/addiction/reducing-stigma)
-homelessness
-incarceration
While attempting to stop illegal drug use, current policies have also contributed to poverty, mass incarceration, and racial disparities. (Vearrier) Harm reduction is designed to decrease HIV transmission and overdose risk while keeping in mind these consequences.
Now, I will be talking about three types of harm reduction used in the U.S. for injection drug use. The first is OEND, or Opioid Overdose Education and Naloxone Distribution. Naloxone is a narcotic that is an antidote for opioid overdose. It is an opioid antagonist, which means that it binds to the sites that opioids usually bind to. Thus, it can reverse or block any effects of other opioids. The point of this harm reduction strategy is to educate people about overdose prevention, what overdose looks like, and what to do in the case of an overdose.
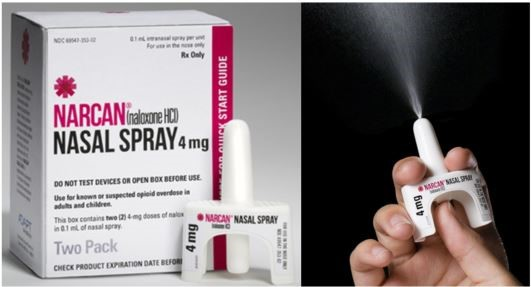
(https://www.co.marion.or.us/HLT/MH/Pages/Narcan-Distribution-Program.aspx)
Next, I’ll talk about the needle and syringe exchange program which many of you have probably heard of before. This program designates sites to collect syringes and dispose of them safely, which is important because diseases such as HIV/AIDS, hepatitis B, and hepatitis C can be spread through this mode. They also provide sterile syringes and other supplies to people. There are 11 official sites in Tennessee and 2 unofficial sites. (Tennessee Harm Reduction)
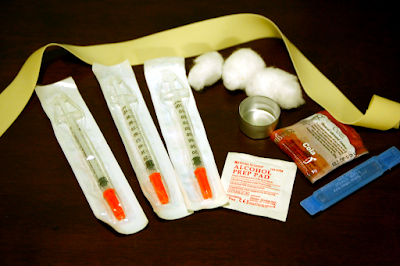 (https://en.wikipedia.org/wiki/Needle_and_syringe_programmes)
(https://en.wikipedia.org/wiki/Needle_and_syringe_programmes)
Now, we'll take a look at opioid maintenance therapy, which is where relatively safer opioids are given to patients who struggle with an opioid use disorder. Methadone and suboxone are longer-acting opiates that are taken orally (safer!). However, a patient can get dependent on both of these, and they do have some street value. There are many regulations in place for these medications to be dispensed. For example, methadone can only be dispensed from specialized clinics, and at the beginning of treatment, patients are actually required to swallow the pills while in the clinic and submit to random urine drug screens and pill counts.
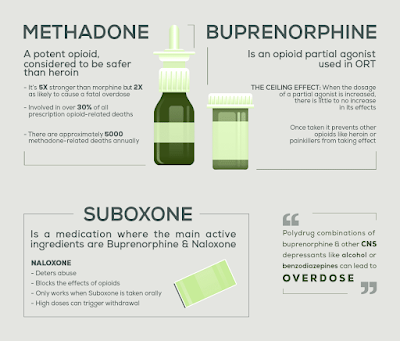
(https://www.northpointrecovery.com/blog/opioid-replacement-therapy-risks-methadone-vs-buprenorphine/)
So now that we’ve talked about these strategies, let’s examine them using the four guiding principles of ethics.
-Autonomy: Yes, we are meeting patients where they are. ("come as you are, and I’ll treat you” & “whether you are using or not, I’ll help you”)
-Beneficence: Yes. This will decrease HIV and overdose risk, doctors get informed consent from patients before prescribing anything, and it decreases the indirect harms associated with drug use.
-Non-maleficence: We could essentially cause harm--a patient could previously be addicted to heroin and now be addicted to or even overdose on methadone. However, we use the equation "total harm = average harm per use x total use" to understand the amount of harm involved. A doctor may have hurt or even led to someone's death with the prescription, but if we look at all the people who have used these opiates and survived many uses because of the prescription, it is good overall.
-Justice: Yes. These harm reduction strategies play a part in eliminating racial disparities and decreasing the amount of people who are incarcerated and houseless.
Now, let’s take this a step further. Let’s talk about two other harm-reduction strategies that are not yet accepted and widely used in the United States. The first is safe injection sites. Basically, safe injection sites provide someone who uses drugs a safe place to come in and use, and there are trained staff present to keep an eye on them. And if they observe signs of overdose, the staff has naloxone on hand and can call for medical help. There are a few of these sites in New York. Per the federal government, the possession of these drugs are illegal, so the sites make a pact with the local law enforcement and agree that these patients will not be prosecuted for possession.

(https://capitalandmain.com/moving-the-needle-science-supports-supervised-injection-sites-why-dont-politicians-agree-1024)
Next, for patients who continue to use heroin despite being prescribed suboxone and methadone, medical-grade heroin can dispensed. There is one site in Canada that does this. What do you guys think about this?
So while the ultimate goal is abstinence, when patients are not able to abstain or are not willing to abstain, rather than ignoring their needs or using punitive measures, harm reduction allows us to meet them where they are and offer some strategies to decrease harm not only to them but also to society.
Some important things to keep in mind are:
1. Getting informed consent
2. Clearly defining the parameters within which these harm reduction strategies will be implemented to minimize risk (train doctors, understand how these treatments work, minimize risk of diversion, minimize risk of overdose)
3. For optimal effects, there may need to be changes to our laws and public opinion so they can go hand-in-hand with the harm reduction strategies we want to implement.
Sources:
Hedrich D, Alves P, Farrell M, Stöver H, Møller L, Mayet S. The effectiveness of opioid maintenance treatment in prison settings: a systematic review. Addiction. 2012 Mar;107(3):501-17. doi: 10.1111/j.1360-0443.2011.03676.x. PMID: 21955033.
Khalid, Farhan et al. “Social Stigmatization of Drug Abusers in a Developing Country: A Cross-Sectional Study.” Cureus vol. 12,9 e10661. 26 Sep. 2020, doi:10.7759/cureus.10661
Marlatt, G.Alan. “Harm Reduction: Come as You Are.” Addictive Behaviors, vol. 21, no. 6, 1996, pp. 779–788., https://doi.org/10.1016/0306-4603(96)00042-1.
Stoljar N. Disgust or Dignity? The Moral Basis of Harm Reduction. Health Care Anal. 2020 Dec;28(4):343-351. doi: 10.1007/s10728-020-00412-y. Epub 2020 Oct 24. PMID: 33098488.
Vearrier L. The value of harm reduction for injection drug use: A clinical and public health ethics analysis. Dis Mon. 2019 May;65(5):119-141. doi: 10.1016/j.disamonth.2018.12.002. Epub 2018 Dec 29. PMID: 30600096.
-bloodborne illnesses (HIV, hepatitis C)
-injection-related bacterial infections (local and systemic)
-overdose complications, including death
Indirect
-violence, homicide, property crime
-involvement in the sex trade
-public stigmatization (It is important to avoid using older, stigmatizing terms when discussing this topic: https://www.bmc.org/addiction/reducing-stigma)
-homelessness
-incarceration
While attempting to stop illegal drug use, current policies have also contributed to poverty, mass incarceration, and racial disparities. (Vearrier) Harm reduction is designed to decrease HIV transmission and overdose risk while keeping in mind these consequences.
Now, I will be talking about three types of harm reduction used in the U.S. for injection drug use. The first is OEND, or Opioid Overdose Education and Naloxone Distribution. Naloxone is a narcotic that is an antidote for opioid overdose. It is an opioid antagonist, which means that it binds to the sites that opioids usually bind to. Thus, it can reverse or block any effects of other opioids. The point of this harm reduction strategy is to educate people about overdose prevention, what overdose looks like, and what to do in the case of an overdose.
(https://www.co.marion.or.us/HLT/MH/Pages/Narcan-Distribution-Program.aspx)
Next, I’ll talk about the needle and syringe exchange program which many of you have probably heard of before. This program designates sites to collect syringes and dispose of them safely, which is important because diseases such as HIV/AIDS, hepatitis B, and hepatitis C can be spread through this mode. They also provide sterile syringes and other supplies to people. There are 11 official sites in Tennessee and 2 unofficial sites. (Tennessee Harm Reduction)
(https://en.wikipedia.org/wiki/Needle_and_syringe_programmes)Now, we'll take a look at opioid maintenance therapy, which is where relatively safer opioids are given to patients who struggle with an opioid use disorder. Methadone and suboxone are longer-acting opiates that are taken orally (safer!). However, a patient can get dependent on both of these, and they do have some street value. There are many regulations in place for these medications to be dispensed. For example, methadone can only be dispensed from specialized clinics, and at the beginning of treatment, patients are actually required to swallow the pills while in the clinic and submit to random urine drug screens and pill counts.
(https://www.northpointrecovery.com/blog/opioid-replacement-therapy-risks-methadone-vs-buprenorphine/)
So now that we’ve talked about these strategies, let’s examine them using the four guiding principles of ethics.
-Autonomy: Yes, we are meeting patients where they are. ("come as you are, and I’ll treat you” & “whether you are using or not, I’ll help you”)
-Beneficence: Yes. This will decrease HIV and overdose risk, doctors get informed consent from patients before prescribing anything, and it decreases the indirect harms associated with drug use.
-Non-maleficence: We could essentially cause harm--a patient could previously be addicted to heroin and now be addicted to or even overdose on methadone. However, we use the equation "total harm = average harm per use x total use" to understand the amount of harm involved. A doctor may have hurt or even led to someone's death with the prescription, but if we look at all the people who have used these opiates and survived many uses because of the prescription, it is good overall.
-Justice: Yes. These harm reduction strategies play a part in eliminating racial disparities and decreasing the amount of people who are incarcerated and houseless.
Now, let’s take this a step further. Let’s talk about two other harm-reduction strategies that are not yet accepted and widely used in the United States. The first is safe injection sites. Basically, safe injection sites provide someone who uses drugs a safe place to come in and use, and there are trained staff present to keep an eye on them. And if they observe signs of overdose, the staff has naloxone on hand and can call for medical help. There are a few of these sites in New York. Per the federal government, the possession of these drugs are illegal, so the sites make a pact with the local law enforcement and agree that these patients will not be prosecuted for possession.
(https://capitalandmain.com/moving-the-needle-science-supports-supervised-injection-sites-why-dont-politicians-agree-1024)
Next, for patients who continue to use heroin despite being prescribed suboxone and methadone, medical-grade heroin can dispensed. There is one site in Canada that does this. What do you guys think about this?
So while the ultimate goal is abstinence, when patients are not able to abstain or are not willing to abstain, rather than ignoring their needs or using punitive measures, harm reduction allows us to meet them where they are and offer some strategies to decrease harm not only to them but also to society.
Some important things to keep in mind are:
1. Getting informed consent
2. Clearly defining the parameters within which these harm reduction strategies will be implemented to minimize risk (train doctors, understand how these treatments work, minimize risk of diversion, minimize risk of overdose)
3. For optimal effects, there may need to be changes to our laws and public opinion so they can go hand-in-hand with the harm reduction strategies we want to implement.
Sources:
Hedrich D, Alves P, Farrell M, Stöver H, Møller L, Mayet S. The effectiveness of opioid maintenance treatment in prison settings: a systematic review. Addiction. 2012 Mar;107(3):501-17. doi: 10.1111/j.1360-0443.2011.03676.x. PMID: 21955033.
Khalid, Farhan et al. “Social Stigmatization of Drug Abusers in a Developing Country: A Cross-Sectional Study.” Cureus vol. 12,9 e10661. 26 Sep. 2020, doi:10.7759/cureus.10661
Marlatt, G.Alan. “Harm Reduction: Come as You Are.” Addictive Behaviors, vol. 21, no. 6, 1996, pp. 779–788., https://doi.org/10.1016/0306-4603(96)00042-1.
Stoljar N. Disgust or Dignity? The Moral Basis of Harm Reduction. Health Care Anal. 2020 Dec;28(4):343-351. doi: 10.1007/s10728-020-00412-y. Epub 2020 Oct 24. PMID: 33098488.
Vearrier L. The value of harm reduction for injection drug use: A clinical and public health ethics analysis. Dis Mon. 2019 May;65(5):119-141. doi: 10.1016/j.disamonth.2018.12.002. Epub 2018 Dec 29. PMID: 30600096.